Medication Administration Record Sheet PDF Form
Medication Administration Record Sheet PDF Form
Inaccurate Consumer Information: Failing to correctly fill in the consumer's name can lead to medication errors. It is essential that the name matches the individual's identification to ensure proper administration.
Missing Attending Physician Details: Omitting the name of the attending physician can cause confusion regarding who prescribed the medication. This information is crucial for accountability and communication among healthcare providers.
Incorrect Medication Hours: Not accurately recording the time of medication administration may result in missed doses or overdoses. Each medication has specific timing requirements that must be adhered to for effectiveness and safety.
Failure to Document Refusals: If a consumer refuses medication, it is vital to document this on the record. Neglecting to do so can lead to misunderstandings about the consumer's adherence to the treatment plan.
Inconsistent Use of Abbreviations: Using abbreviations without a clear understanding of their meanings can create ambiguity. It is important to ensure that all staff are familiar with the abbreviations used in the record.
Neglecting to Record Changes: Failing to document any changes in medication, such as dosage or frequency, can compromise patient safety. Any modifications should be clearly noted to maintain an accurate record.
The Medication Administration Record Sheet (MAR) is an essential tool in healthcare for tracking medication administration. It shares similarities with several other documents used in medical settings. Below is a list of nine documents that are comparable to the MAR, highlighting their similarities.
When filling out the Medication Administration Record Sheet form, attention to detail is crucial. Here are ten essential guidelines to follow and avoid.
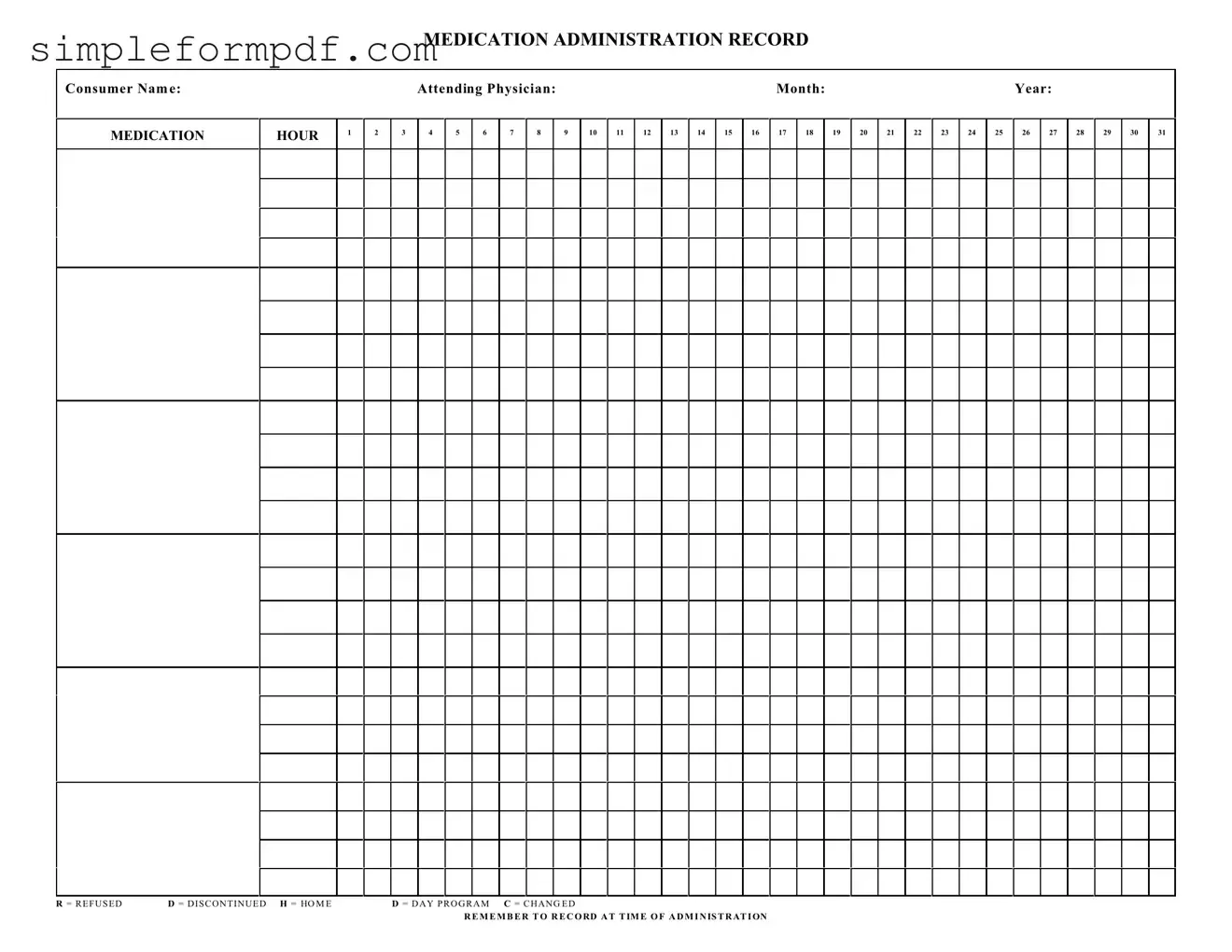
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
Contractor Proposal Form - Can stipulate the materials and methods to be used.
By using a Georgia Durable Power of Attorney form, individuals can ensure that their financial matters are handled as they wish, even in the event of their incapacity. For those considering this important legal step, templates and resources can be found at georgiaform.com, providing guidance on how to effectively set up this document.
Printable Daily Cash Drawer Count Sheet - Track cash sales and cash payments seamlessly with this form.
Understanding the Medication Administration Record (MAR) Sheet is crucial for ensuring proper medication management. However, several misconceptions can lead to confusion. Here are some common misunderstandings:
By addressing these misconceptions, individuals involved in medication administration can improve accuracy and safety in healthcare settings.
Filling out the Medication Administration Record Sheet is an essential task that ensures accurate tracking of medication administration for individuals in care. This process requires careful attention to detail to maintain clear and precise records. Below are the steps to effectively complete the form.